Fistula-in-Ano Treatment Methods
Learn More About Your Treatment
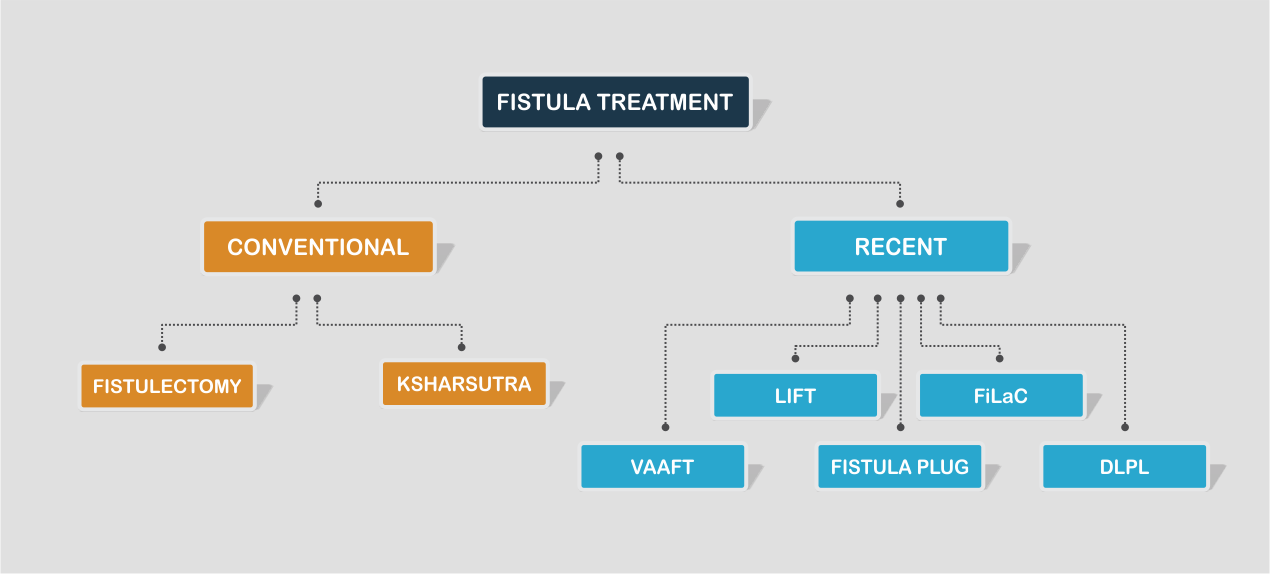
I. FISTULECTOMY
This is a surgical procedure in which the fistula tract is completely excised. Done under Spinal or General anaesthesia, the fistula tract is removed and the groove that is formed is left behind to heal. This procedure carries with it the risk of damage to the sphincter muscle resulting in fecal incontinence and is usually reserved as a treatment option for Complex fistula.
At Noble Surgicare Hospital, Laser is used as an adjunct to Fistulectomy to minimize the risk of damage to the sphincter muscle. Thus, with the added advantage of Laser the chances of post-operative incontinence are negligible.
II. KSHARSUTRA
This is an ancient Ayurvedic technique in which a special thread is used to treat the fistula. This thread is coated with Ayurvedic preparations and is inserted into the fistula tract.
The local irritation caused by the alkaline thread causes chemical cauterisation leading to inflammation within the tract. As a result the tract begins to debride. An important action of the Ksharsutra is that it allows continuous drainage of pus and debris from the tract. As all the infected material is drained, healing begins in a clean environment.
Advantages of Ksharsutra
- Non-invasive technique. Therefore no cuts and stitches.
- No damage to the sphincter muscle
- Fairly good success rate.
Potential drawbacks of Ksharsutra
- Multiple weekly sessions of treatment needed. So it’s a long treatment that is completed over a few months.
- The thread is a source of irritation. So there may be persistent local burning and pain.
- It is comparatively less effective in recurrent and complex fistulas.
III. VAAFT ( Video Assisted Anal Fistula Treatment )
The VAAFT technique is used for the surgical treatment of Complex fistulas. It is performed with the use of a fistuloscope. The procedure consists of 2 phases
- Diagnostic stage: In this phase your surgeon will identify the external opening of the tract through which the scope is introduced. Once this is done, the entire tract and any accessory tracts are delineated.
- Treatment stage: During this phase the inner side of the tract is fulgurated from the internal opening towards the external opening. This is followed by cleaning of the tract and closing the external opening.
Advantages
- No surgical wounds on the buttocks or perianal region.
- The internal opening is precisely located which is important in the treatment of any fistula.
- No damage to the sphincter muscle
Potential drawbacks
- The biggest argument against VAAFT is its high rate of recurrence (~30%)
IV. LIFT ( Ligation of Interspincteric Fistula Tract )
This procedure is usually performed for Complex or Deep fistulas. A seton is first placed in the fistula tract, forcing it to widen over time. A few weeks later, the surgeon removes the infected tissue and closes the internal fistula opening. The advantage of this procedure is that the fistula is accessed between the sphincter muscles thus avoiding cutting them. However, the success rate of LIFT is ~70% with an impaired healing in 20-30% cases.

V. FISTULA PLUG
The fistula plug is a 100% synthetic bio-absorbable scaffold. This plug is placed in the fistula tract. Over time cells from the body migrate into the scaffold and new tissue is generated as the body gradually absorbs the plug material, leaving no permanent material in the body.
Advantages of Fistula Plug
- No cutting involved and no operation wound. Therefore it is associated with less pain and faster recovery.
- No damage to the sphincter muscle.
Potential Drawbacks
- Failures can occur due to dislodgement of plug from the fistula tract.
- The plug can get infected
- Failure of treatment can occur in 25-30% cases
VI. FiLaC ( Fistula-tract Laser Closure )

This procedure, done using the Lesotronics Laser. The aim of the procedure is to gently remove the fistula tract without damaging the sphincter muscle.
The procedure is done under Spinal or short General Anaesthesia and requires about 30-40 minutes. A radially emitting Laser Fibre is inserted from the outside. A defined amount of laser energy is then emitted circumferentially into the fistula tract. The laser energy causes controlled photothermal destruction of the fistula tract causing it to collapse to a high degree. This also helps supports and accelerates the healing process.
Advantages of FiLaC
- It has an excellent healing rate as compared to all other techniques.
- The anal sphincter is preserved so there is no risk of post-operative incontinence.
- It can be done in complicated fistulas like recto-inguinal, recto-gluteal fistulas.
- It is safe in high risk patients like those with hypertension, cardiac ( heart ) problems and in senior citizens.
Potential drawbacks of FiLaC
- There may be local burning for some time
- Post-operative subcutaneous abcess : It is usually managed with medications and dressing.
- In rare cases it may need incision and drainage under local anaesthesia.
VII. Distal Laser Proximal Ligation ( DLPL )
Fistula is a complex disease. Ultimately the aim of any fistula treatment is not just to get rid of the existing fistula but:
1. To save the sphincter muscle and thus prevent incontinence.
2. To prevent recurrence, considering the nature of the disease
Most of the techniques like VAAFT, LIFT, FiLaC achieve the primary purpose of closing the fistula and saving the sphincter. However, they all have their own rates of recurrence. Considering how bothersome a fistula is, even a small chance of recurrence can be a concern for the patient.
Dr Vishal Pawar, having specialised in Proctology ( a branch of surgery which deals with the rectum and gluteal region), has treated a large number of Fistula cases. In his experience of treating fistula patients over the past years, he tried to understand the nature of the disease and the cause of recurrences. After an in-depth study and applying all his knowledge and skills, he devised a technique he has labelled DLPL – Distal Laser Proximal Ligation.
In this procedure any abcess cavity along with the internal opening is first excised.This is followed by closure of the distal tract. The proximal part of the fistula tract is then sealed with the Leonardo Laser. With the radially emitting fibre of the laser, energy is applied circumferentially to the fistula tract. This ensures complete closure of the tract.
IN HIS SERIES OF 100 PATIENTS WITH COMPLEX HIGH FISTULAS TREATED WITH DLPL, THERE WAS NOT A SINGLE CASE OF RECURRENCE OR INCONTINENCE.
3D Endo-anal Imaging
Recently introduced 3D Endo-anal Pelvic Floor Imaging is an highly advanced, established technique for imaging the rectum and anal canal. It is rapid, simple and well-tolerated. It also provides valuable information about the anatomy of the anal sphincters.
Role of 3D Endo-anal Imagining in Fistula
Many patients suffering from Fistula are not diagnosed properly because of the complex anatomy and limited diagnostic options. Although MRI Fistulogram is a commonly used technique for Fistula imaging, many patients are claustrophobic or just fear getting inside the MRI machine. Besides, Fistula is a dynamic disease wherein new tracts and abscesses may form from time to time. Thus an old MRI may not give an accurate picture of the current disease. 3D Endo-anal Pelvic Floor Imaging is a patient-friendly procedure that can be done at any given time. The most important aspect of this technique is that it can be used intra-operatively, which means that the surgeon can use it while performing the surgery. Post-operatively, it is used to confirm the accuracy of the fistula repair.
India’s latest 3D Endoanal Imaging for Fistula/Abscess
3D Endoanal Imaging is an important tool to study the various characteristics of Fistula. Fistulae are visualised as hypoechoic tracts. Specific features like the site of internal opening, level of the radial tract, the relation of tracts to anal sphincters and site of fluid collections/pararectal cavities can be obtained. It provides a detailed multiplanar reconstruction of the anal canal. 3D Imaging is particularly helpful in high fistulae with anal sphincter involvement, especially if there are additional extensions and associated pararectal collections. It gives useful information about the sphincter defects which is important in planning surgery in order to minimise damage to anal sphincter complex.

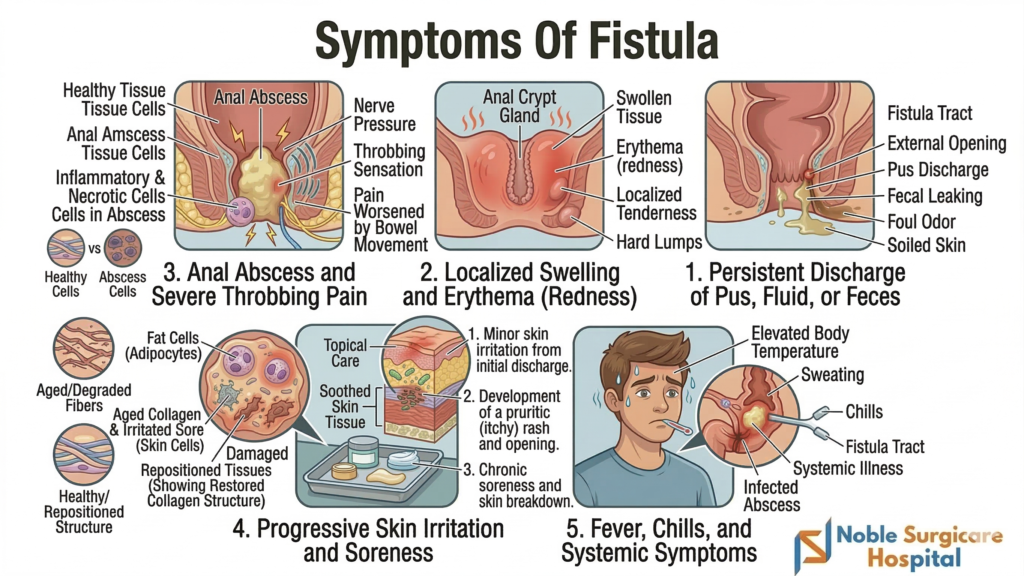
Types of Fistula